Printable Form Cms 1763
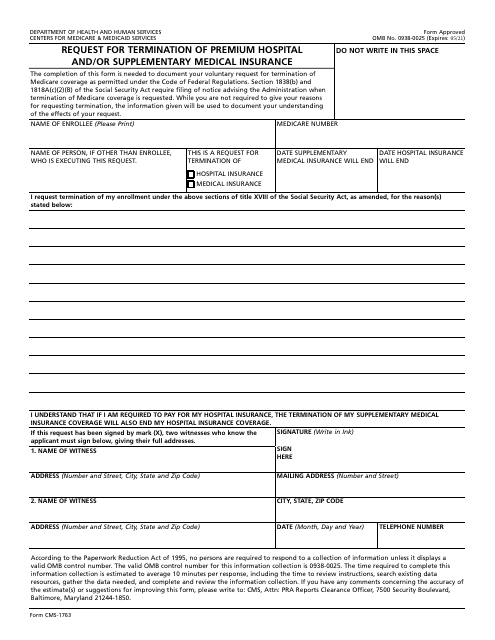
Printable Form Cms 1763 - Web form approved omb no. All you need is smooth internet connection and a device to work on. Customize your document with our simple tools. Web what situations qualify for an exceptional conditions special enrollment period? Follow the simple instructions below: People with medicare premium part a or b who would like to terminate their hospital or medical. Create your esignature and click ok. Use fill to complete blank online medicare & medicaid pdf forms for free. Save, download, share, print or send for signature. Therefore, we do not offer. Signing up for part a & part b if you meet the criteria for a special enrollment period. Get everything done in minutes. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Select the document. Don't delay, try for free today! Web a person who has expressed a wish to stop their medicare coverage will be accountable for paying for their hospital insurance. This is allowed under title xvii of the social security act. Customize your document with our simple tools. Web form approved omb no. Save or instantly send your ready documents. All you need is smooth internet connection and a device to work on. Therefore, we do not offer. Signing up for part a & part b if you meet the criteria for a special enrollment period. Enjoy smart fillable fields and interactivity. Web hi 00820.901 exhibit 1: It becoming increasingly more prominent amongst organizations of all sizes. However, with our preconfigured online templates, everything gets simpler. Don't delay, try for free today! Get everything done in minutes. They are also a simple way to get data from your customers. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Select the document you want to sign and click upload. Web free cms 1763 template. The completion of this form is needed to document your voluntary request for termination. People with medicare premium part a or b who would like to terminate their hospital or medical. Enjoy smart fillable fields and interactivity. Select the document you want to sign and click upload. Web cms 1763 printable form63? Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. This is a request for termination of. Web a person who has expressed a wish to stop their medicare coverage will be accountable for paying for their hospital insurance. Customize your document with our simple tools. Save, download, share, print or send for signature. Check out how easy it is to complete and esign documents online using fillable templates and. Select the document you want to sign and click upload. Web the cms 1763 form is a legal issued by the centers of medicare and medicaid services that allows medicare recipients to terminate their coverage of premium hospital insurance (premium part a) and/or supplemental medical insurance (part b). This is a standard department of health and human servicesform it is. Web this form is used to terminate the hospital and or medical insurance benefits you receive from medicare. All you need is smooth internet connection and a device to work on. Create your esignature and click ok. They are also a simple way to get data from your customers. Who can use this form? The information you are submitting in the paper is confidential. A typed, drawn or uploaded signature. Therefore, we do not offer. All forms are printable and downloadable. Web name of enrollee (please print) medicare claim number name of person, if other than enrollee, who is executing this request. Select the document or form you need create. Create your cms 1763 in minutes! The centers for medicare & medicaid services (cms) requires, when possible, a personal interview be conducted with everyone who wishes to terminate entitlement. Save, download, share, print or send for signature. Easily fill out pdf blank, edit, and sign them. Web hi 00820.901 exhibit 1: 05/21) request for termination of premium hospital and/or supplementary medical insurance. Once completed you can sign your fillable form or send for signing. Web what situations qualify for an exceptional conditions special enrollment period? Web name of enrollee (please print) medicare claim number name of person, if other than enrollee, who is executing this request. Web thanks for your question. Select the document you want to sign and click upload. Web 21 votes how to fill out and sign form cms 1763 online? It becoming increasingly more prominent amongst organizations of all sizes. The form cannot be completed by cms staff. This is a standard department of health and human servicesform it is for use by any medicare enrollee who wants to stop receiving premium hospital (medicare part a) and supplementary medical insurance (medicare part b). Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. All you need is smooth internet connection and a device to work on. Get everything done in minutes. Create your esignature and click ok. Its comprehensive collection of forms can save your time and enhance your efficiency massively. The centers for medicare & medicaid services (cms) requires, when possible, a personal interview be conducted with everyone who wishes to terminate entitlement. This is a request for termination of. Web form approved omb no. Easily fill out pdf blank, edit, and sign them. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. The form cannot be completed by cms staff. Get your online template and fill it in using progressive features. Save, download, share, print or send for signature. Web name of enrollee (please print) medicare claim number name of person, if other than enrollee, who is executing this request. The information you are submitting in the paper is confidential. Web cms 1763 printable form63? Create your esignature and click ok. Follow the simple instructions below: This is allowed under title xvii of the social security act. Decide on what kind of esignature to create.
Medicare, Social Security, and Form CMS 1763 PDFfiller Blog
Where Do I Mail Medicare Form Cms 1763 Form Resume Examples AjYdXvKoYl
Where Do I Mail Medicare Form Cms 1763 Form Resume Examples AjYdXvKoYl

Where Do I Mail Medicare Form Cms 1763 Form Resume Examples G28BAjpr3g

Social Security Medicare Form Cms 1763 Form Resume Examples jl10DJW012
Gio Workers Compensation Claim Form Nsw Form Resume Template
Form CMS1763 Download Fillable PDF or Fill Online Request for

Medicare Hospital Stay 3 Days Social Security Medicare Forms
Form CMS1763 Download Fillable PDF or Fill Online Request for
Social Security Medicare Form Cms 1763 Form Resume Examples wRYPwQW394
Don't Delay, Try For Free Today!
Web This Form Is Used To Terminate The Hospital And Or Medical Insurance Benefits You Receive From Medicare.
Therefore, We Do Not Offer.
Who Can Use This Form?
Related Post: